So here we all are, on the other side. I survived the procedure. I guess that I should apologise for leaving you all hanging. Since leaving hospital I have had a few things going on with friends and family. And, keeping a blog going does require a degree of concentration and effort. Of which I have had none.
My procedure, I am very pleased to say went well, took place on Monday 31st March. Originally estimated to take 4 – 4.5 hours, actually took six hours. On regaining conciousness, in the recovery room, I was given two pieces of news.
Firstly, that they, the surgical team, had taken more than was originally planned. Originally, I was supposed to be having a “left hemicolectomy” but in the end I had an “extended right hemicolectomy”.
Secondly, a bit of very welcome news, was that I did not have a stoma and therefore would not be having to deal with a colostomy bag.
The Hospital Stay
After a brief sojourn in the recovery room I was wheeled along to ICU to spend my first night in hospital. But before I could contemplate sleep I was given a full body bed bath. That was a first for me.
I was also starving, not having eaten since Sunday evening, the day before. But at this time I was restricted to clear fluids.
How noisy are hospitals ? Staff banging cupboard doors, clattering of trolleys and trays and let’s not forget talking at elevated levels. At one stage there was a guy strutting the length of the ward, and back again, speaking into a phone which he held away from his face.
Don’t they realise there are sick people in ICU, trying to rest and recover ?
1st April – Operation Day +1
At around 10:30 the staff in ICU got me out of bed, had me sitting in a chair and brought me stuff to have a wash. To be fair I didn’t stay in that chair for long. It was too upright, not very comfy, made my back ache and my tummy was a bit sore.
But there was a nice view away to the south and west looking out over Portchester, the Isle of Wight and down to Southampton Water. All with blue skies and sunshine.
Still no food, just clear fluids, black tea, black coffee, water !!! and I’m starving.
Later, on the evening of the same day, they moved me out of ICU and shipped me off to the surgical ward. Sharing the ward with six other inmates and no view.
If I thought ICU was noisy, they had nothing on this ward. I couldn’t see what it was but there was something at the far end of the ward making a sound like a diesel truck on a fast idle. Thankfully after about thirty minutes it stopped. Rumour has it that the noise was from an air bed being inflated !!!
Apart from the noise, another issue I had was the temperature of the ward. On arrival I broke into a sweat and I know, when at home, I break out at around 25°C. One of the nurses very kindly brought me a fan which improved things but, under cover of darkness, someone snuck in and turned it off.
How Rude!
2nd April – Operation Day +2
A nurse brought me a bowl of warm water for a wash and a change of gown. Ablutions completed I tried to put on the fresh gown which was way to small. When I flagged the size issue I was told that they had no gowns my size and offered me a “shirt”, i.e. an NHS pyjama jacket which was even smaller. The nurse said she would order a larger gown.
Order ? How long was that gonna take?
Anyway, thankfully, someone turned up with a large gown. I should point out that I did have my own pyjamas but due to the various tubes attached about my person there was no way I could get into them. At this time I was catheterised and also having a saline drip.
Time in hospital can pass very slowly. I had prepared for this by bringing in a book to read, also a book of crossword puzzles. I also had my phone on which I do soduku and read via Kindle. The problem was that I couldn’t focus on anything. In fact trying to focus took so much effort I kept dozing.
I had a very pleasant visit from my granddaughter in the morning and, later, my wife and daughter arrived to break up the afternoon.
At last, I was told I could have something to eat. My first meal for three days was a supper of chicken soup, yoghurt, jelly, and vanilla ice cream. Not very substantial but you would not believe how good that chicken soup tasted.
Throughout the day, with each and every visit from a nurse or doctor, I was constantly asked if I have moved my bowels, or if I have broken wind. At this time my answers were all in the negative.
After supper I was asked what I wanted for brekky. Options were orange juice and/or yoghurt. I opted for the yoghurt.
3rd April – Operation Day +3
I had a visit from the surgeon. Nice guy. He introduced himself and I promptly forgot his name. He said he wanted to try me on real food, with more substance. He also said they were planning to remove the catheter… yay!! Also, there was mention of the possibility of me going home, either today or tomorrow. This is all sounding good. All of this was discussed while he tapped, squeezed, and generally fondled my belly. Oh, I didn’t mention the gaggle of other medics, around half a dozen, gathered around the foot of my bed. Any privacy or dignity I had rapidly flew out the window.
I was given some of my own daily blood pressure meds. I’ve not had any since before the op. I was also given a dose of liquid paracetamol. It is thick in texture, very sweet and it tastes of strawberries, Yuuukkk !!!
I don’t remember lunch but supper was Pea Soup with an awful bread roll. Think the roll was made without any fat, it fell apart when I tried to cut it so that I could butter it. Tried eating it but it just clagged up my mouth. There was also an egg mayo sandwich. I only ate half as it was on some strange, strongly flavoured, malted bread, and again a weird texture. I tried dunking it in the soup but it didn’t help. Obviously my tastebuds had become confused. Hospital food isn’t really that bad. or is it?
During the day I have been getting an acidic feeling at the back of my throat, like indigestion. I mentioned this to a nurse who got me some Gaviscon. It helped a bit.
4th April – Operation Day +4
Bad news, I’ve been sick!! I was told that if I am sick twice in the day I will be aspirated i.e. have a tube put up my nose and down into my stomach. This sounds unpleasant, and definitely something to be avoided.
Now they are taking bloods to see if I have an infection, and are concerned about the low volume pee. So, I definitely won’t be going home today.
Supper time arrives and I was feeling sick and requested another anti-sickness pill. Supper was chicken soup but I don’t recall eating it.
Even though I’m just drinking water it seems to be sitting high in my tummy. I’m not feeling comfortable at all.
5th April – Operation Day +5
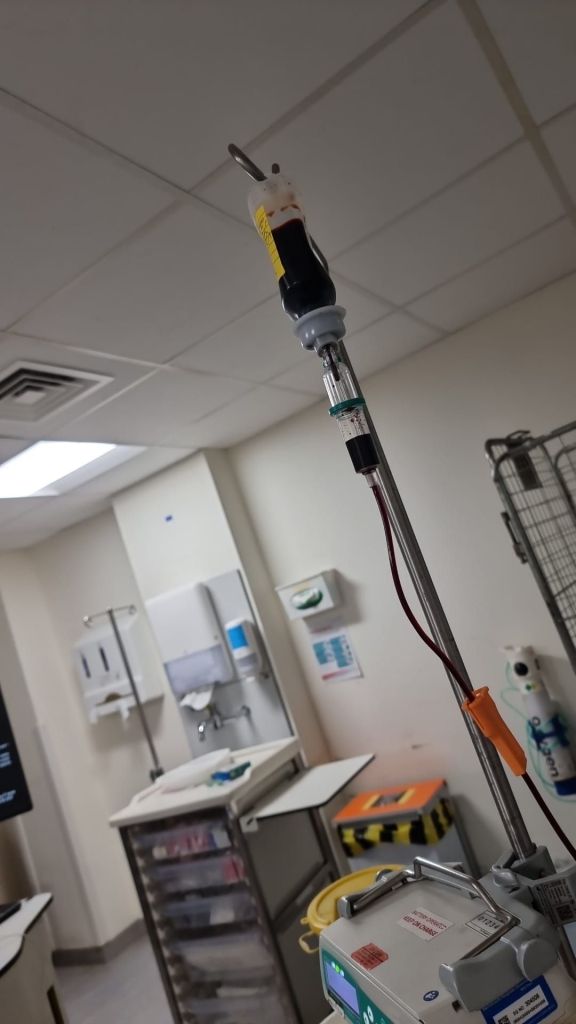
So, I was sick during the night and as a result I was intubated. That was not a pleasant experience. As the tube goes in it causes you to retch and then once inserted you can feel the tube in your throat every time you swallow. The nurse siphoned out nearly a litre of dark green fluid. It appears that my vomiting is due to Ileus, a not uncommon post operative complication after abdominal surgery. In essence the bowel goes on strike
So now I have two bags hanging on the side of the bed. One for my catheter and one for my nasal tube. I also have a saline drip attached to the cannula in my right arm. It’s almost like being at the centre of a spiders web.
While the tube is in I am nil by mouth, just sips of water. So back to my starvation diet.
6th April – Operation Day +6
Due to all my attachments I had to call for the commode last night. And, whilst sat on the commode, my nasal tube took it upon itself to sneak out and fall on the floor. I buzzed for the nurse who got a fresh tube and installed it which again caused me to retch and vomit. Just wonderful. That was at 03:00.
During the day they disconnected my nasal tube from its bag and told me I could go on free fluids. So I had an ice cold glass of milk, and boy did that hit the spot. The milk was, later, followed by a cup of hot chocolate.
I was told that I can stay on free fluids but they will reconnect the tube to the bag at night time. Some good news, it was confirmed that Bovril is allowed under the free fluids plan so have asked Gerry to bring some in.
Bad news, the blood tests have shown some negative markers, and so, they think I might have developed an infection. Therefore, as a precaution, I have been moved to my own room. Bonus, I have my own window with a view and can open said window, so plenty of fresh air.
In the early evening I had a lovely video call from my granddaughter and her kids. Jax, who is autistic, saw my nasal tube and immediately wanted to know what it was. We told him I was in hospital. His response was “go get Grandad, bring him home” Unseen by me, Jax trotted off downstairs, let himself out the front door and was trying to get into his mums car. Their dog, Milo, alerted my daughter and she caught him outside. Cute.
7th April – Operation Day +7
Thankfully the nasal tube has been removed and so, it appears, I’m back on the free fluids diet which is some kind of progress. Lunch today was tomato soup, orange jelly, and vanilla ice cream, bliss!!!
In the afternoon, friends, Eric, Mary, and Mo visited for a couple of hours. It was nice to have someone to talk to. Eric and Mary left after an hour which left Mo to entertain me. Unfortunate for Mo, she was soon treated to the sight of me sliding out of bed clutching the back of my gown, carrying my bag of urine (golden handbag) and shuffling across the corridor to the loo. She took it all in good heart.
Todays supper treat was mushroom soup, more jelly, and ice cream. The soup was, once again, very tasty.
After Mo’s departure and having nothing better to do, I read the ingredient list for the orange jelly. Shock, horror, there is no orange in it. There is carotene, I assume that’s for the colour. I had thought that the flavour was a little odd, now I know why.
8th April – Operation Day +8
Finally, I got a decent night’s sleep, the first since the surgery. Also, my tummy is feeling less bloated which, I guess, means some of the gas used during the operation is beginning to dissipate.
Brekky today was rice crispies, orange juice, toast, and marmalade. Actually, to call it toast was a bit of an exaggeration. I think the slice of bread had seen a photo of a toaster but not actually been in one. Still, after being starved and then only getting liquids to eat this was definitely a step up and in the right direction.
After breakfast I was asked to select my lunch, so I chose Beef Lasagne, scallop potatoes and gravy. More solids … yes!!!
The lasagne was blooming marvellous although, surprisingly, I had to confirm that it was beef, to me it tasted like the best herby pork sausage. So that has triggered the idea that I will try making a lasagne with italian pork sausage meat, when I get home.
I also had a bit of a revelation today. I had a shower, my first since prior to my surgery, and I was so pleased to get my hair washed. The whole shower thing was a bit weird as I still had the catheter in place and so I had to take my golden handbag along with me. But sitting on the provided stool and just letting the water flow over me was superb.
I also had lots of visitors today, so it was a good job that I had that shower … lol.
Todays supper was Lancashire hotpot with extra mash. The hotpot was very nice but the mash was very dry. And, I didn’t get the recommended extra gravy I requested. However, I did get two Vanilla ice creams. They really are very nice, smooth and creamy.
Finally, my catheter has been removed but, unfortunately, I haven’t pee’d since. So I was given an ultrasound of the bladder and, apparently, there wasn’t much pee in there so retention isn’t an issue. Bottom line, I have to up my fluid intake, then if I don’t pee they will catheterise me again. And we don’t want that.
With the catheter gone I am now in my jim jams which are much more comfortable than those horrible hospital gowns. And finally, at around 21:00, the dam burst and I managed a pee. This was followed by several others during the night. All were captured so the nurses could check the volume and, apparently, all is good.
9th April – Operation Day +9
Hallelujah, the surgeon has told me that I can go home, shook my hand and wished me well. I asked a nurse what the discharge procedure was. I was told that getting meds from the pharmacy was usually the thing that dictated when I could go, but that I should expect late afternoon or evening.
Shortly after this the ward sister came to see me, told me my meds had been requested and the indications were that they would be available sooner, rather than later. She told me to order lunch just in case it actually was later. In fact meds and lunch arrived together. I was told to have lunch and then the discharge process could be completed.
Wow, lunch was a celebration. Roast turkey breast, roast potatoes, sprouts, carrots, and, wait for it, banana stuffing!!!! Who ever heard of banana stuffing? Certainly not me, and it wasn’t for my palate. Apparently, it is a carribean thing.
Anyway, food eaten, sister returned with my meds, my discharge papers and one last bit of education. New news to me was that I was going to have to inject myself with an anticoagulant. She had a syringe and rolled up pad to simulate my tummy. I was directed in the correct use. The two carrier bags of meds contained, primarily, several boxes of preloaded syringes. I am to inject myself twice daily, for thirty days.
So, formalities completed, the porter arrived and I was soon loaded into a wheel chair and propelled to the main exit where my son-in-law was waiting to drive me home.
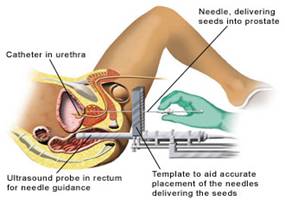
And there we have it. My hospital experiences around my robotic laparoscopic right side hemicolonectomy.